- G
- G
- K

Just a few weeks ago Brandon and Monica’s world was turned upside-down. What started out to be an exciting 19/20 week growth ultrasound and gender reveal, turned into baby Clark’s diagnosis of CDH. In the following weeks Monica and Brandon have been educating themselves on CDH, and trying to prepare for what is to come. There will be lots of decisions to be made and a possible temporary relocation of their family, in order to give baby Clark the best possible care. With all the unknowns associated with CDH and this endeavor; we (the Family of Brandon and Monica) are reaching out to ask for help, which is never an easy thing, then again, neither is their situation. Your donations will be used to help afford the cost of travel, food, housing, medical bills, and all the other bills that incur while this little guy’s family spends precious time with him in the NICU. Please know that ANY donation helps and that no amount is too small, every penny counts. And any of your prayers and positive thoughts sent their way are also very much appreciated. Thank you for taking the time to read about baby Clark’s journey, and thank you for helping us in any way that you can, we are eternally grateful. <3 –Baby Clark’s Cheerleaders

What is CDH?
Congenital Diaphragmatic Hernia (CDH) occurs in approximately 1 in every 2,500 births (1,600 cases in the U.S. each year). The cause of CDH is not yet known. The diaphragm is formed in the first trimester of pregnancy and controls the lungs' ability to inhale and exhale. CDH occurs when the diaphragm fails to form or to close totally and an opening allows abdominal organs into the chest cavity. This inhibits lung growth.
When the abdominal organs are in the chest, there is limited room for the lungs to grow. This prevents the lungs from developing normally, resulting in pulmonary hypoplasia (or underdeveloped lungs). This can cause reduced blood flow to the lungs and pulmonary hypertension (high blood pressure in the pulmonary circulation), as well as asthma, gastrointestinal reflux, feeding disorders and developmental delays.
Every patient diagnosed with CDH is different. Survival rates depend on the types and number of organs involved in the herniation and the amount of lung tissue available. There are many surgical procedures and complications that may or may not occur with each individual.
The fact is, roughly 50% of babies born with CDH do not survive. Of the 50% that do survive, most will endure long hospital stays, feeding issues, asthma and other problems. A few of the survivors suffer from severe long-term medical issues. However, we already know baby Clark is a fighter so these odds won’t scare him.
CDH occurs as frequently as Spina Bifida and Cystic Fibrosis, yet there is very little research being done and virtually no media coverage.
Treatment
Baby Clark’s care for CDH has already started, a team of doctors are closely monitoring him and his mama’s pregnancy. With frequent exams, ultrasounds, cardiac echo’s, and even CT scans. His care will become especially critical in the last trimester, at 34 weeks ultrasounds increase to weekly. This close monitoring will help to determine if it is necessary to deliver early.
Every baby with CDH is different - like a snowflake, no two are alike. Babies born with CDH, every little detail matters and can impact the outcome. In addition to surgical repair, baby Clark may require specialized equipment such as the oscillator ventilator, heart lung machine (ECMO), or nitric oxide. Because of this, it is important that baby Clark is delivered in a hospital with immediate access to this equipment if necessary.
The delivery
At the time of delivery the Neonatal Surgical Team — including neonatologists, surgical advanced practice nurses, neonatal and surgical fellows, neonatal surgical nurses, and Respiratory Therapists will all be waiting to stabilize baby Clark and provide any specialized ventilation (breathing) assistance before bringing him to the NICU for further care.
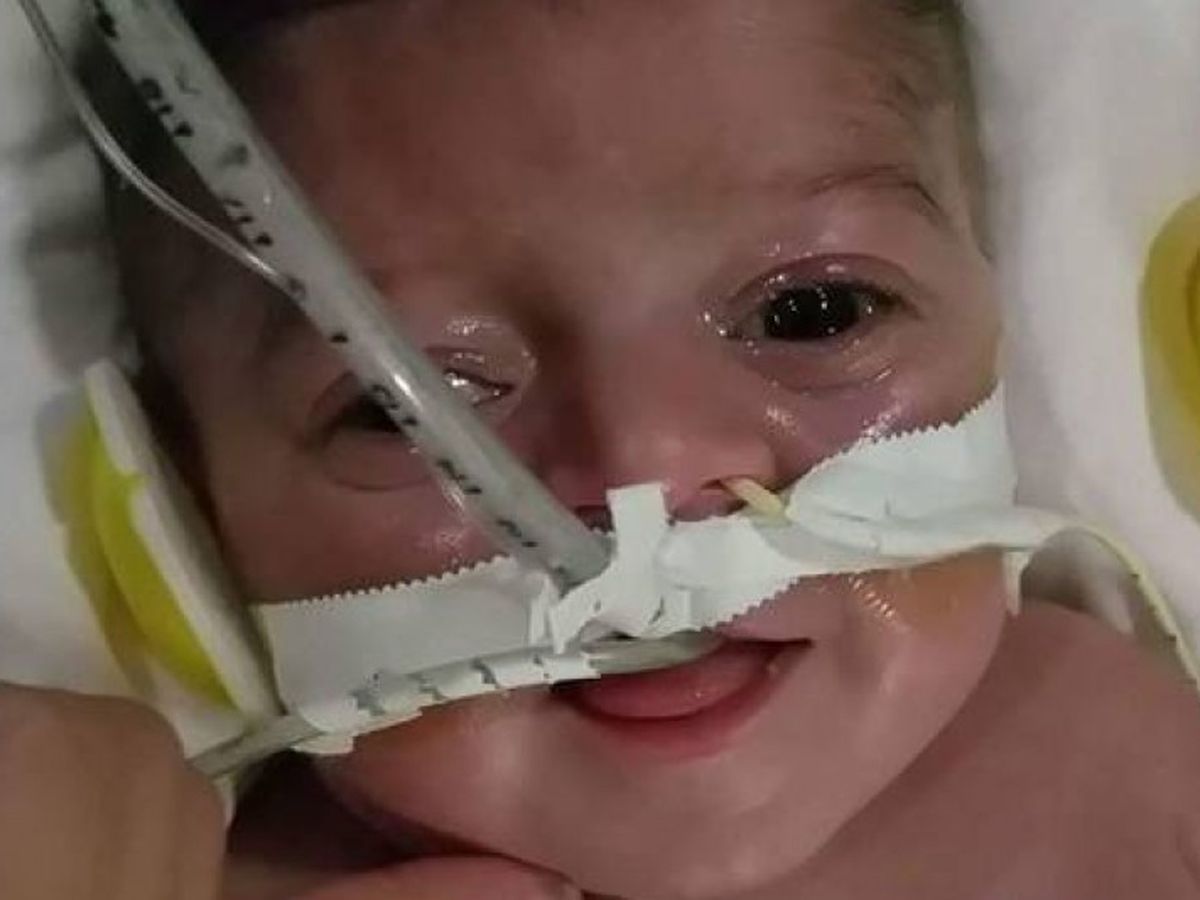
At stabilization, a breathing tube is inserted into his airway so a ventilator can be attached to help with breathing. A tube going from the mouth or nose to the stomach will be placed to keep air from getting into the stomach and intestines causing less space for the lungs to expand. Intravenous and arterial lines will be placed in blood vessels in his arms, legs or belly button for administration of fluids and medications. Blood gases will be drawn from the arterial line to assess how well he is oxygenating.
What is ECMO?
Babies with severely compromised or fragile lungs may require extracorporeal membrane oxygenation (ECMO), a temporary bypass technique used to oxygenate the blood and allow the lungs to rest. Under sterile conditions, the pediatric surgeon will place two tubes called cannulas into the artery and vein in baby Clark’s neck. The tube in the neck takes blood out of the body from the large vein, oxygenates the blood through the ECMO circuit and returns the now oxygenated blood to the baby by the carotid artery. ECMO is used when other treatments are unsuccessful. The lungs rest as the ECMO circuit does the work. In some cases the baby may have the CDH repair while on ECMO.
What happens during surgery?
Surgical repair of CDH depends on each baby’s progress in the days following birth, and can occur as early as three days of life (It is typical to let the baby stabilize and become comfortable on the ventilator before surgery is attempted.). An incision is made just below the rib cage, the organs in the chest are guided back down into the abdomen and the hole in the diaphragm is sewn closed. The space created in the chest allows the lungs to continue to grow; Baby Clark's lungs will continue to grow and develop more air sacs or alveoli all the way through his early childhood.
What does the future look like?
Long-term follow-up by a team of experts is important to provide the best clinical care for this little guy. Children with CDH require comprehensive, interdisciplinary follow-up care. The team is made up of clinicians from general surgery, developmental pediatrics, pulmonary, cardiology, psychology, nutrition, audiology, social services and others as needed. Initial follow-up will be arranged when baby Clark is in the NICU. Appointments are tailored to each child’s needs, but typically occur at 6 months, 12 months, 2 years, 4.5 years and 6 years, and then every 2 years thereafter, as needed. Appointments are designed for visits to multiple specialists in one day.
Organizer and beneficiary
Brandon Clark
Beneficiary